Encephaloceles and Cerbrospinal Fluid Leaks of the Ear
Overview:
The normal ear contains many air spaces that serve a role in how the ear functions as it transmits sound from the outside world to the delicate inner ear nerve structures. Although these air spaces are a normal part of every healthy ear, they do create voids into which surrounding structures (i.e. the brain) can expand if the bony barrier is not strong enough to resist it.
The brain lives on top of and behind the ear. It is surrounded by a membrane known as the dura. Within that dura is an important liquid known as cerebrospinal fluid (CSF). This fluid bathes the brain and maintains a constant pressure of at least 10-18 cm H20 at all times. This constant pressure creates an outward push into areas of less resistance, such as the air containing voids of the ear. In some patients the CSF pressure becomes even higher, such as in those who are obese or have obstructive sleep apnea (OSA).
If there are weak areas of bone between the ear and the brain, this constant pressure can push the dura and the brain into the ear. These weak areas in the bone may be present from birth or slowly develop over time as a person ages. They can also be the result of chronic ear infections or of the prior ear surgery needed to treat such infections.
The vast majority of such problems occur from above the ear and therefore involves the temporal lobe of the brain pushing down into the ear. When the brain becomes pushed into the ear it is known as an encephalocele. This is a brain “hernia” so to speak. It does not harm the brain when this happens, and the portion of brain that does herniate into the ear is not what is important.
What is important is when this encephalocele stretches the dura to a point that it breaks and the CSF leaks into the ear. Also the herniating brain can impinge upon the mechanical structures of the ear and impede sound transmission. Often the patient notices pressure in the ear or hearing loss. When seen by a doctor, they either have fluid behind the ear drum or a mass that looks like a tumor. Some ENT doctors may put an ear tube into the ear to relieve the fluid, only to have it drain an unending supply of clear watery fluid.
A small encephalocele that is not leaking CSF and that does not cause any hearing loss, does not necessarily require aggressive treatment. However, an encephalocele that is causing hearing loss, or that causes ear pressure symptoms, or that is leaking CSF does require treatment. This is because infection can easily spread into the CSF whenever there is not a good barrier to prevent it. Such an infection is known as meningitis and is life-threatening.
Diagnosis:
Commonly patients with a CSF leak present to an ENT doctor’s office with fluid behind the ear drum that will not go away with medicine treatment. If the doctor is keenly aware of the potential for a CSF leak, he/she can have the patient lean far forward with the face looking down at the floor. In some patients with a CSF leak, drops of clear fluid may run out of the nose as it runs out of the ear down the Eustachian tube.
Usually the doctor will place a tube in the eardrum, which is commonly done for other forms of chronic ear fluid. However in the case of a CSF leak, the fluid will be found to be very clear and watery as opposed to yellowish or mucous type fluid that is usually found when ear fluid is due to other causes. With a tube in place, the patient with a CSF leak often finds that the ear drains profusely and without end, although the quantity may wax and wane. A cotton ball placed into the ear can become so saturated that drops of fluid can be wrung out of it after a few hours. If the CSF leak is slow, the fluid will mainly be noticed when the patient sleeps at night, waking up with a large wet spot on their pillow.
Fluid collected from the ear or the nose can be sent for a test known as beta-2-transferrin to confirm that it is CSF. This if often unnecessary since the diagnosis should be apparent based on clinical presentation.
A plain CT scan of the ear is a very important part of the evaluation. It can identify any missing areas of bone between the ear and the brain through which the leak is most likely occurring. Often an encephalocele is easily visualized. However, in cases where the entire ear space is also filled with CSF, it can be difficult to distinguish between CSF and the size of the encephalocele. The anatomy information provided is essential nonetheless.
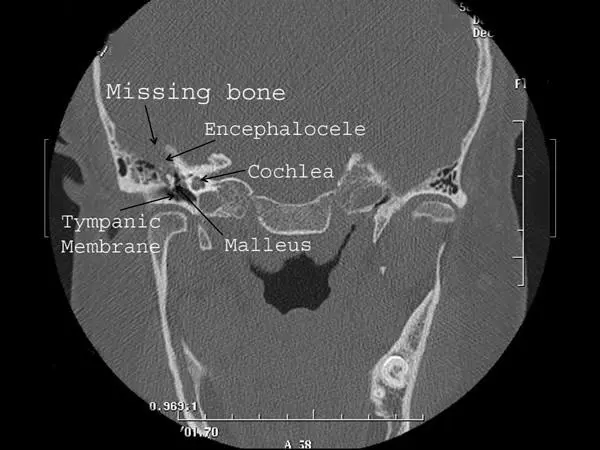
CT scan image of a right ear encephalocele as viewed from the front of the patient. On this CT image bone is white, brain tissue and CSF are gray, and air in the ear is black.
A CT cisternogram involves placing a radiographic contrast dye into the CSF through a spinal tap, followed by performing a CT scan. This test can often show the dye entering the ear, confirming a CSF leak. However it does not provide much additional useful information. Therefore we find CT cisternograms mostly unnecessary in the treatment of this condition.
MRI scans are obtained preoperatively in patients for whom surgery is planned to repair an encephalocele or CSF leak. An MRI can distinguish between brain tissue and CSF in the ear, better demonstrating the size of the encephalocele. However, they do not provide any useful information about the bony anatomy. They are mostly obtained to be sure there are no other intracranial abnormalities about which we need to be aware.
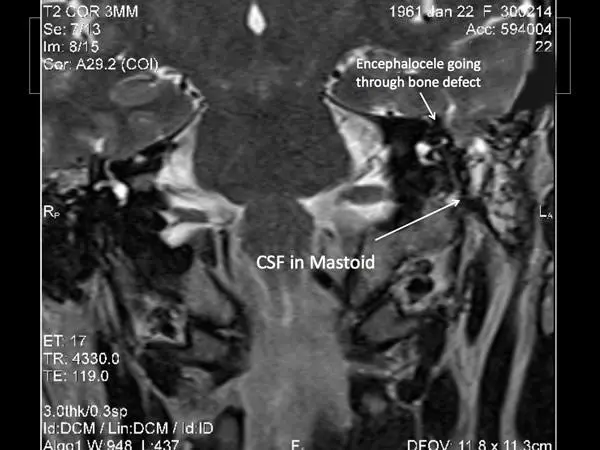
MRI scan of encephalocele in a left ear as viewed from the front of the patient. On an MRI image of this type bone is black, brain tissue is gray, and CSF is bright white.
TREATMENT:
So how is an encephalocele or CSF leak in the ear best treated? There are no medications that can fix an ear encephalocele or CSF leak once it has developed. Surgery is the only option.
In the past, the gold standard of surgical repair has been to approach the problem from above, through a temporal craniotomy or “middle fossa” approach. This is a very major neurosurgical operation, but does allow for repair of any holes in the floor of the middle cranial fossa (which is the roof of the ear) and for strong repair of the dura so that it does not leak. It has the advantage of not requiring any disassembly of the hearing bones of the middle ear. Unfortunately this surgery also requires an extended stay in the neuro ICU, a long recovery period, and a prolonged amount of time off work. In addition, elderly patients do not do well with this approach. This approach is still sometimes required in more extreme cases.
At the Dallas Ear Institute, we have worked diligently to develop techniques to repair the majority of ear encephaloceles and CSF leaks via an “ear” approach. Such an approach allows this to be a “day surgery” repair with no stay in the hospital and with limited time off of work. In addition, this is a much more effective approach for older patients who would not be able to tolerate the extremes of a middle cranial fossa approach.
Transmastoid (through the ear) repair of encephaloceles and CSF leaks is successful in over 90% of patients. It is so successful that I recommend it as the first treatment approach in all patients.
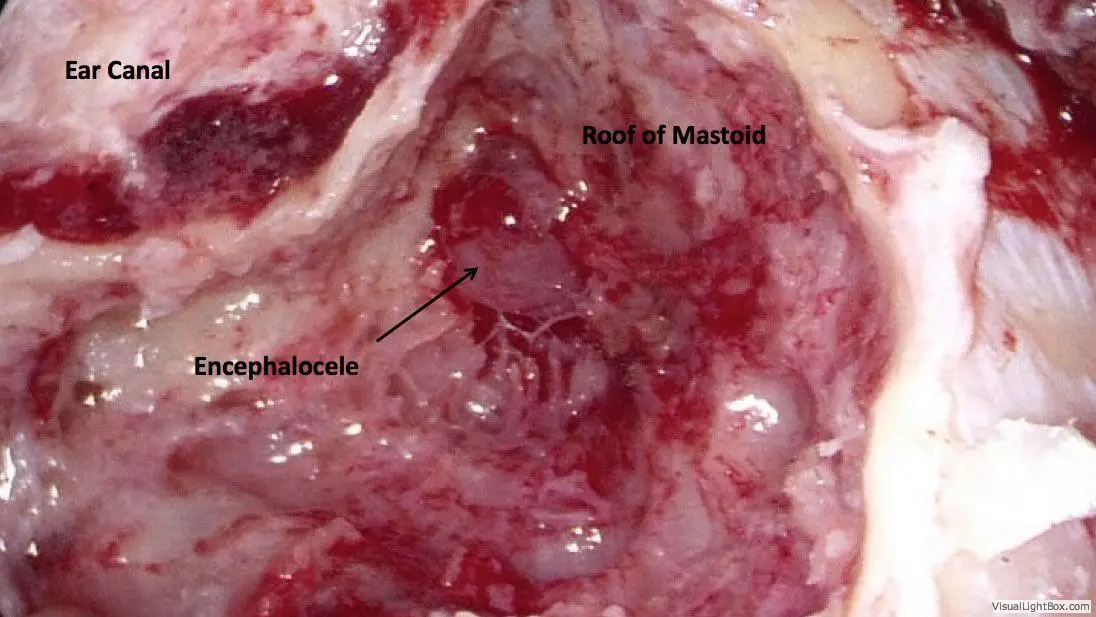
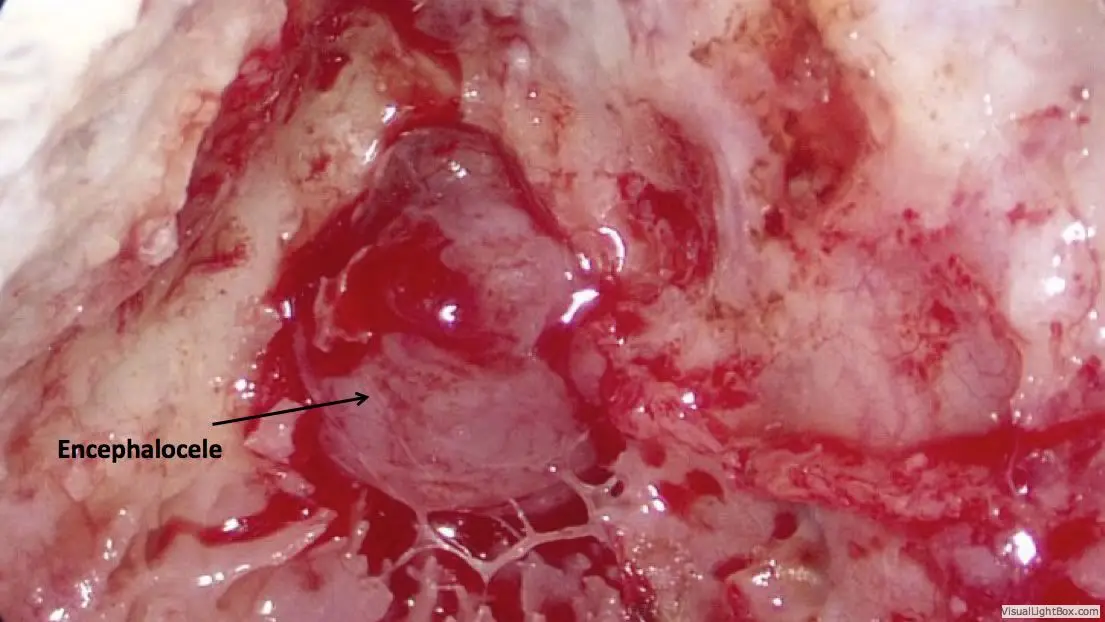
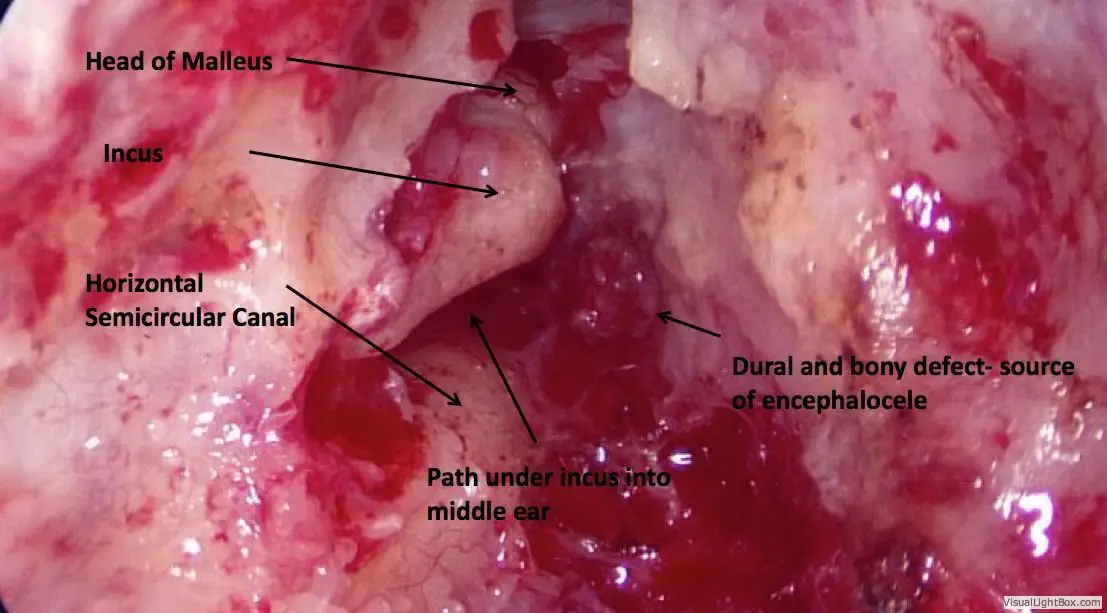
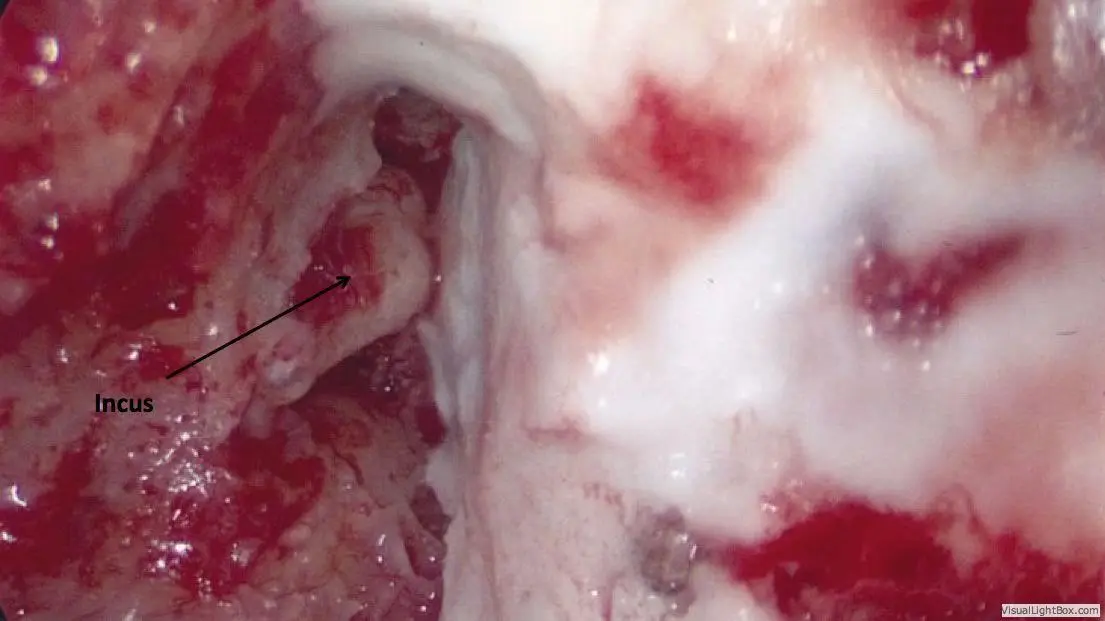
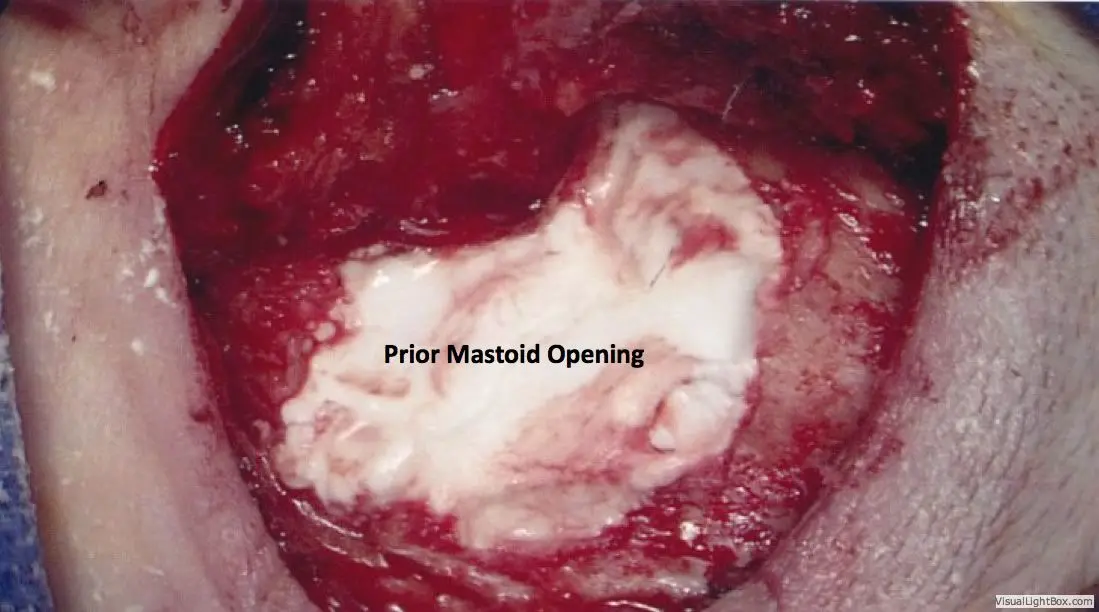
General anesthesia is required. Practically no hair is shaved. An incision is made hidden in the crease behind the ear, through which the entire surgery can be performed. The mastoid air space is opened with a drill, providing access to nearly the entire roof of the ear. Whatever brain is hanging down into the ear is removed using a bipolar cautery device. This does not result in any neurologic deficit, since the brain tissue contained in the encephalocele is non-functional anyway.
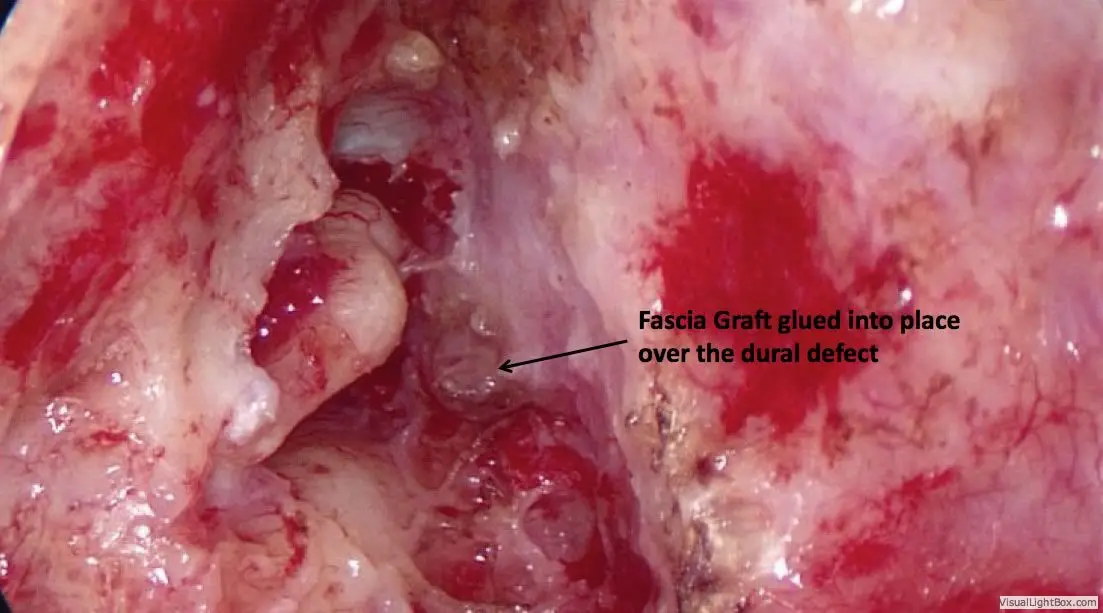
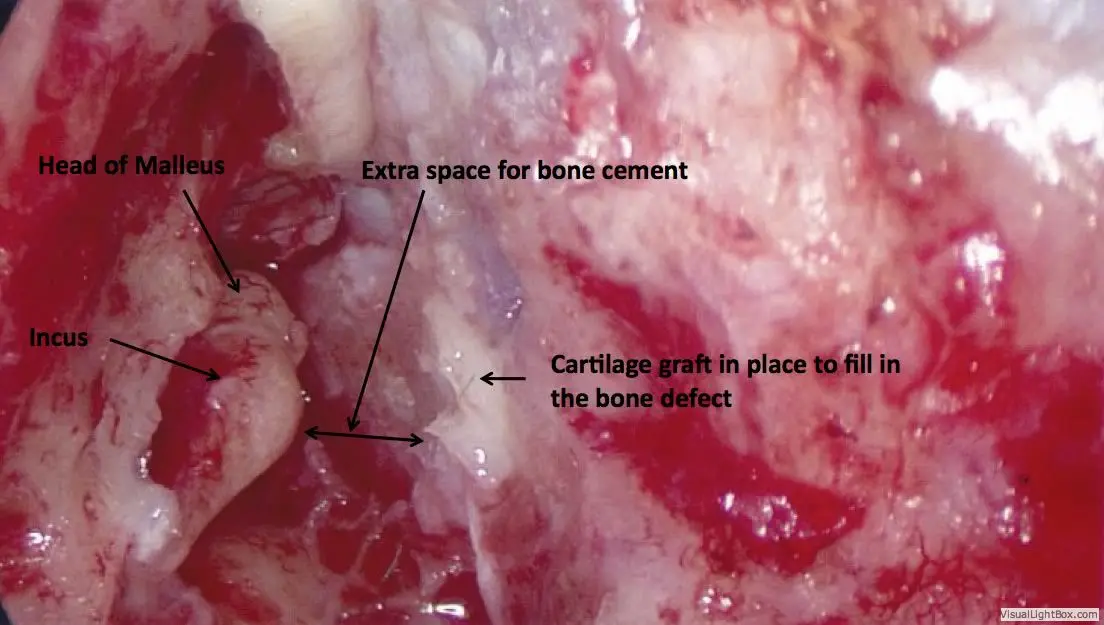
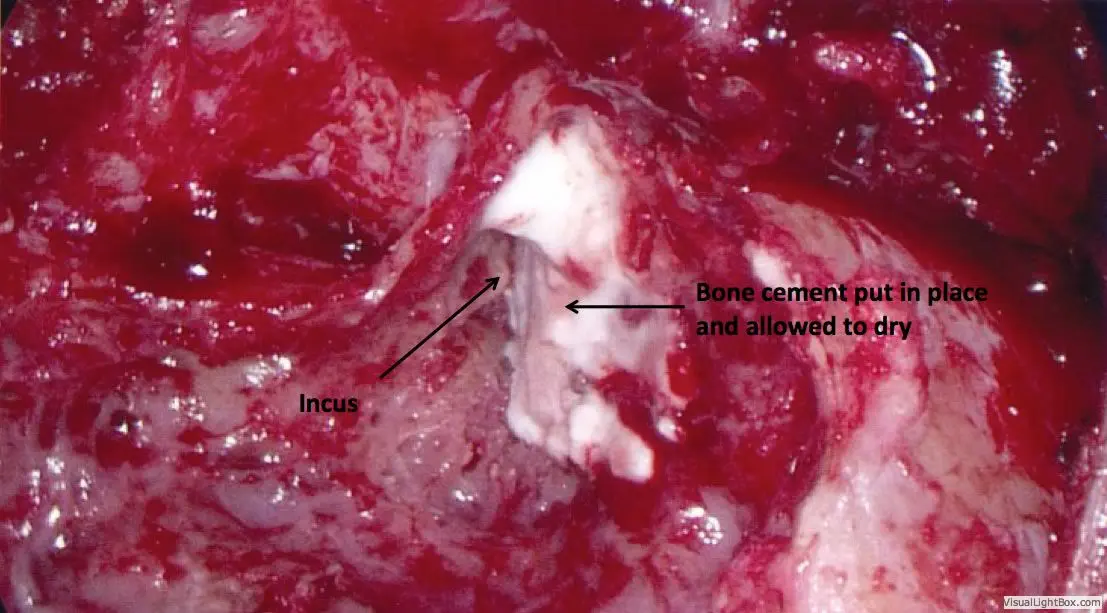
Once the encephalocele is removed, the dural defect through which it has herniated is repaired with the patient’s fascia tissue and special adhesives. The bone defect is then repaired using the patient’s own ear cartilage. There is plenty of cartilage that can be used without affecting the appearance of the ear. Once this is in place, the entire defect is then additionally reinforced with bone cement.
Depending on the location of the defect, the patients hearing bones may have to be disassembled so that the repair can be performed thoroughly. After the repair is complete, the hearing bones are then reassembled. This process may result in a 5-10% hearing loss, but the hearing can still be quite good.
The patient is discharged home a few hours after surgery and can usually return to work within a few days. However it is important that the patient not do any straining or aggressive sports activity for 6-8 weeks.
SUMMARY:
Acquired ear encephaloceles and CSF leaks are common. It is estimated that the frequency of this condition is increasing due to the increasing incidence of obesity and obstructive sleep apnea in our population.
At DEI we now take a streamlined approach to diagnosis and treatment. If the patient’s clinical presentation is typical for an encephalocele/ CSF leak, the only necessary diagnostic tests are a plain CT scan of the ear and an MRI scan. With this information we can proceed with surgery in the majority of cases. The transmastoid approach allows for direct visualization of the problem and for a secure repair using modern techniques as well as advanced adhesives and bone cements. Complications and morbidity are very low in experienced surgical hands, much less than with the temporal craniotomy approach.